
When the first vaccine against COVID-19, the BNT162b2 vaccine (Comirnaty®, manufactured by BioNTech/Pfizer) based on mRNA technology, became available to the general public in very early 2021, it was prioritized for elderly citizens above the age of 80 Germany. This was in the middle of the third wave which was dominated by the B.1.1.7 (“UK”) variant of SARS-CoV-2.
It was an informal discussion in January 2021 between professor Michael Lohoff, chair of the microbiology department at Philipps University Marburg and myself, head of the Marburg University Hospital virus diagnostic laboratory, both trained immunologists: we felt that it would be relevant – and have societal implications – to develop and focus a research project on the specific immunity issues related to age. Also, after research had focused on the evolving virological properties of SARS-CoV-2 during the first waves, immunology questions would now become even more burning with the advent of vaccine availability. We were highly interested in the group of elderly people above the age of 80, who are most susceptible to COVID-19 infection and thus most dependent on the novel vaccine. We aimed for a study that would recruit and follow a cohort of 50-60 participants.
Getting started
But how? In January 2021, local vaccination centers were getting constructed. Marburg is a small university town with 70,000 inhabitants, located in the center of Germany, and has many advantages due to its small size: Distances are short, both between places and between people, thus facilitating administrative set-up of our study. We convinced our friend and colleague Henrik Mei at the German Rheumatism Research Center (DRFZ) in Berlin to collaborate as expert in deep immunological phenotyping. Together, we established a T cell stimulation protocol that utilizes peptide pools spanning the entire spike protein of SARS-CoV-2: Selecting T cells that up-regulate CD40L and produce IFN-gamma upon antigenic (in our case spike proteins) stimulation by flow cytometry, we were able to measure even very small T cell frequencies among blood-derived lymphocytes, with high specificity and a neglectable background.
Within about six weeks, all administrative details could be fixed: We received enthusiastic support from the local authorities and the vaccination center in Marburg, where we started to recruit elderly participants mid-March 2021. It was a fortunate coincidence that one of my former students had just graduated from medical school and worked at the local vaccination center, which facilitated the study organization. By April 2021, we obtained funding from the state of Hesse. Blood samples were taken at the vaccination center before first and second vaccination. Since most of our elderly participants came from very rural parts of our district, mobility was an issue – so the third samples were taken during a scenic early-summer home visit tour by students and senior investigators to people’s homes.
We made the experience that our participants were highly motivated to participate in the study, so there we had virtually no dropouts. Recruitment of younger participants, who obtained access to the vaccine much later than elderly people, took place in May 2021 in a local general practitioner’s clinic.
Data gems
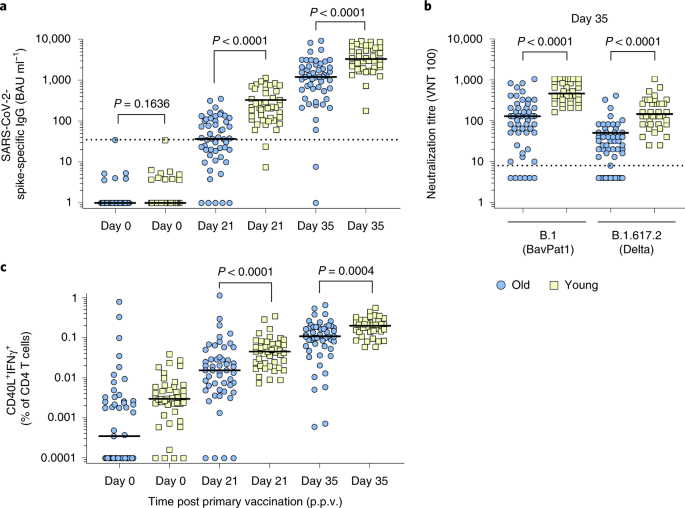
Hypothesizing that age matters for SARS-specific immunity, we observed already after the very initial analyses of T cell and antibody data after first vaccination that there were striking age-dependent differences in SARS-CoV-2-specific immunity: about a half-log difference in T cell frequencies and one log difference in antibody concentrations between young and elderly vaccinees. When we finalized the data analysis post-second vaccination in summer 2021 and looked at a correlative plot with antibody and T cell responses, we observed that the immune response among young participants was very homogeneous, but among our elderly donors, about 10% of individuals were poorly responsive (Fig. 2B). We could exclude that they were generally weak responders to microbial antigens by demonstrating robust responses toward staphylococcal enterotoxin B by T cells and sustained antibody levels against measles and varicella-zoster virus.
The identification of five low-/non-responders prompted us to prepare a third vaccination for five individuals which were assumed to have an only weak degree of protection. Again, we received help from the local vaccination center and health authorities, since at that time a third vaccination was a very premature approach.

discussing study results with colleagues
I remember very well when my student sent me the data on third vaccination – it was while I spent a weekend at the countryside with my family where we had a pretty bad phone network that made it pretty difficult to communicate. These data principally showed an unexpected booster effect in those who had a pretty weak primary response – a glimpse of hope for our vulnerable target group?
From here, it became clear that we had to involve our colleagues in virology who were able to perform virus neutralization tests. During the review process of our paper, the Delta variant (B.1.617.2) emerged, and we were able to demonstrate and include an increase of Delta-specific neutralization after third vaccination.
Retrospective
From the availability of vaccination via submission of the ethics proposal, assay set-up, funding and sample collection, it took us about half a year from scratch to obtain these data, and another three months until data were published upon peer-review. The rather personal environment of a small university town made it possible to conduct this study as a collaborative bottom-up project. We are grateful for the sustained motivation of our elderly participants to continue their contribution to the study, and we are still in close contact with them. Without their and their families’ support, this study could not have been realized.
We learned that in elderly individuals, the immune response induced by the novel mRNA vaccines can differ considerably, and that immunoassays addressing T cell-mediated and antibody-mediated immunity are useful to identify poor responders in this vulnerable age group. Our study group was among the first to communicate the usefulness of a third vaccine in elderly people to policy makers on the state and federal levels. We think that our study will also impact the next vaccine generations.




Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in